Insights for AI Builders
Encord Blog

All articles
398 of 398 articles
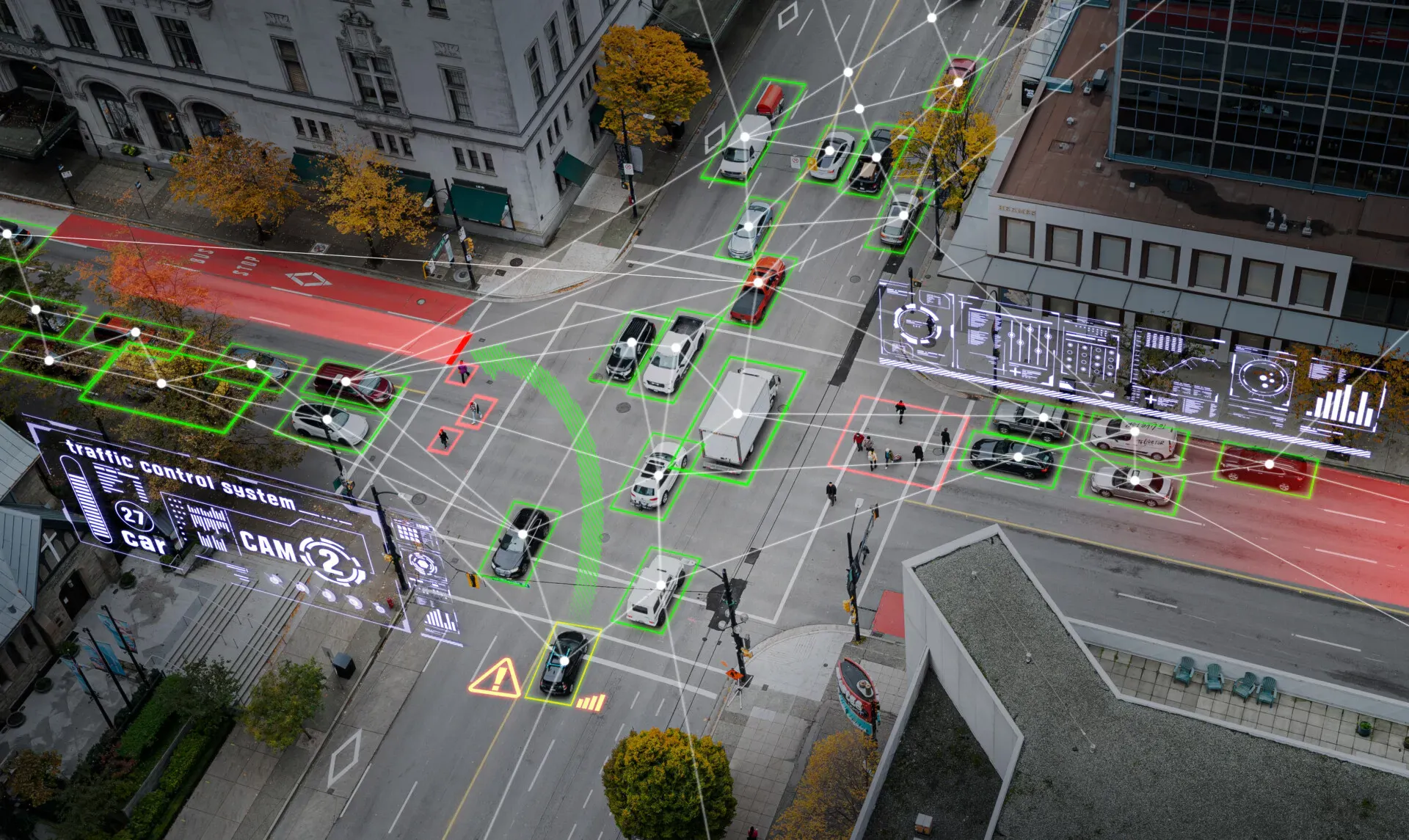
Smart city computer vision: A practical guide to training data
Smart cities
Aug 04 2026
How to Build Diverse Egocentric Datasets for Robotics: A Practical Guide
Physical AI
Jul 30 2026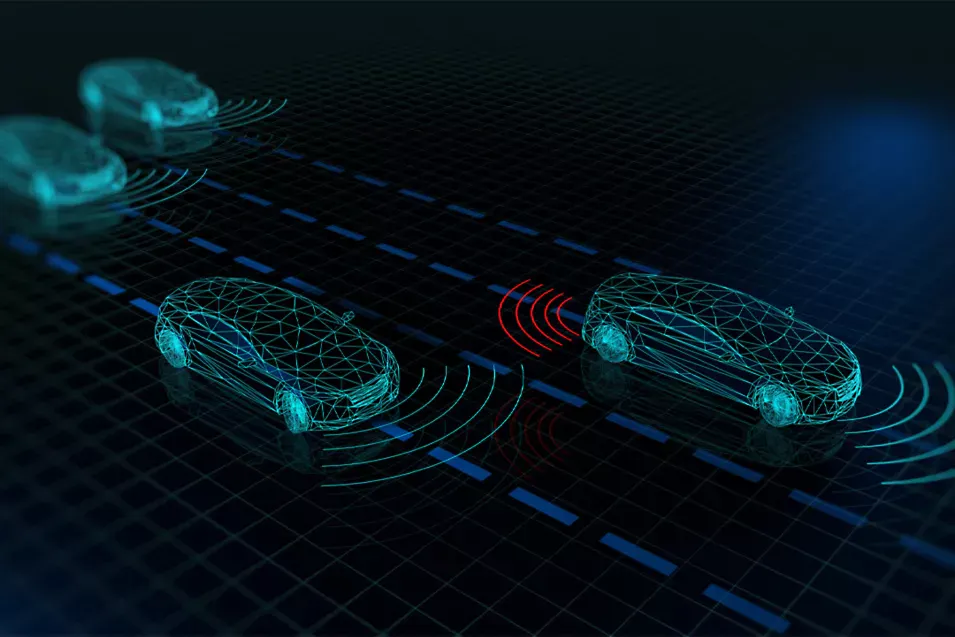
Sensor Fusion Data Annotation: How to Label Multi-Sensor Robotics Data
Data Annotation
Jul 29 2026
Full Guide to Building an Autonomous Vehicle Training Dataset
Data Annotation
Jul 28 2026
Bounding Box vs. Polygon vs. Segmentation vs. Keypoint: Which Annotation Type Fits Your Task?
Image Annotation
Jul 23 2026
FDA's New Predetermined Change Control Plan Rule for Radiological AI Software, Explained
Healthcare
Jul 17 2026![The Eval Stack the Top AI Teams Are Building Right Now [Webinar Recap]](https://images.prismic.io/encord/Ofy3UdJLjLvH-X_S_AICircle_webinarbanner_speakers.jpg?auto=format%2Ccompress&fit=max)
The Eval Stack the Top AI Teams Are Building Right Now [Webinar Recap]
Model Evaluation
Jul 17 2026
How to annotate video for ADAS and autonomous driving: A Technical Guide
Smart cities
Jul 15 2026
How to annotate video for machine learning: A Step-by-Step workflow
Video Annotation
Jul 13 2026
You Don't Have a Data Problem. You Have a Curation Problem
Data Curation
Jul 10 2026
AI Data Curation for LLM and Multimodal Teams: A Practical Framework
Data Curation
Jul 09 2026
Data Curation Best Practices for AI: A Step-by-Step Framework
Data Curation
Jul 09 2026